


 Sign Out
Sign Out

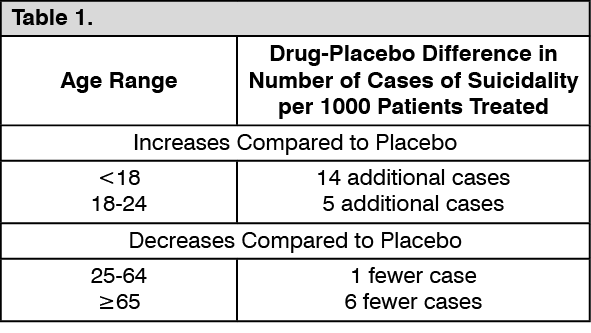
The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive-compulsive disorder (OCD) or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4,400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk differences (drug vs placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1,000 patients treated) are provided in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNo suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was not sufficient to reach any conclusion about drug effect on suicide.
It is unknown whether the suicidality risk extends to longer-term use ie, beyond several months. However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression.
All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality and unusual changes in behavior, especially during the initial few months of a course of drug therapy or at times of dose changes, either increases or decreases.
The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania and mania, have been reported in adult and pediatric patients being treated with antidepressants for MDD as well as for other indications, both psychiatric and non-psychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.
Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset or were not part of the patient's presenting symptoms.
Families and caregivers of patients being treated with antidepressants for MDD or other indications, both psychiatric and non-psychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior and the other symptoms described previously, as well as the emergence of suicidality, and to report such symptoms immediately to healthcare providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for Wellbutrin XL should be written for the smallest quantity of tablets consistent with good patient management, in order to reduce the risk of overdose.
Neuropsychiatric Symptoms and Suicide Risk in Smoking Cessation Treatment: Wellbutrin XL is not approved for smoking cessation treatment, but bupropion under the name Zyban is approved for this use. Serious neuropsychiatric symptoms have been reported in patients taking bupropion for smoking cessation (see Adverse Reactions). These have included changes in mood (including depression and mania), psychosis, hallucinations, paranoia, delusions, homicidal ideation, hostility, agitation, aggression, anxiety and panic, as well as suicidal ideation, suicide attempt and completed suicide. Some reported cases may have been complicated by the symptoms of nicotine withdrawal in patients who stopped smoking. Depressed mood may be a symptom of nicotine withdrawal. Depression, rarely including suicidal ideation, has been reported in smokers undergoing a smoking cessation attempt without medication. However, some of these symptoms have occurred in patients taking bupropion who continued to smoke. When symptoms were reported, most were during bupropion treatment, but some were following discontinuation of bupropion therapy.
These events have occurred in patients with and without preexisting psychiatric disease; some have experienced worsening of their psychiatric illnesses. All patients being treated with bupropion as part of smoking cessation treatment should be observed for neuropsychiatric symptoms or worsening of preexisting psychiatric illness.
Patients with serious psychiatric illness eg, schizophrenia, bipolar disorder and MDD did not participate in the premarketing studies of Zyban.
Advise patients and caregivers that the patient using bupropion for smoking cessation should stop taking bupropion and contact a healthcare provider immediately if agitation, depressed mood or changes in behavior or thinking that are not typical for the patient are observed, or if the patient develops suicidal ideation or suicidal behavior. In many post-marketing cases, resolution of symptoms after discontinuation of Zyban was reported, although in some cases the symptoms persisted, therefore, ongoing monitoring and supportive care should be provided until symptoms resolve.
The risks of using bupropion for smoking cessation should be weighed against the benefits of its use. Zyban has been demonstrated to increase the likelihood of abstinence from smoking for as long as 6 months compared to treatment with placebo. The health benefits of quitting smoking are immediate and substantial.
Screening Patients for Bipolar Disorder: A major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled trials) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described previously represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder and depression. It should be noted that Wellbutrin XL is not approved for use in treating bipolar depression.
Bupropion-Containing Products: Patients should be made aware that Wellbutrin XL contains the same active ingredient found in Zyban, used as an aid to smoking cessation treatment, and that Wellbutrin XL should not be used in combination with Zyban or any other medications that contain bupropion eg, Wellbutrin SR or Wellbutrin, the immediate-release formulation.
Information for Patients: Patients should be advised that taking Wellbutrin XL can cause mild pupillary dilation, which in susceptible individuals, can lead to an episode of angle closure glaucoma. Preexisting glaucoma is almost always open-angle glaucoma because angle closure glaucoma, when diagnosed, can be treated definitively with iridectomy. Open-angle glaucoma is not a risk factor for angle closure glaucoma. Patients may wish to be examined to determine whether they are susceptible to angle closure and have a prophylactic procedure (eg, iridectomy), if they are susceptible.
Seizures: Bupropion is associated with a dose-related risk of seizures. The risk of seizures is also related to patient factors, clinical situations and concomitant medications, which must be considered in selection of patients for therapy with Wellbutrin XL. Wellbutrin XL should be discontinued and not restarted in patients who experience a seizure while on treatment.
As Wellbutrin XL is bioequivalent to both the immediate-release formulation of bupropion and to the sustained-release formulation of bupropion, the seizure incidence with Wellbutrin XL, while not formally evaluated in clinical trials, may be similar to that presented as follows for the immediate-release and sustained-release formulations of bupropion.
Dose: At doses up to 300 mg/day of the sustained-release formulation of Wellbutrin SR, the incidence of seizure is approximately 0.1% (1/1,000).
Data for the immediate-release formulation of bupropion revealed a seizure incidence of approximately 0.4% (ie, 13 of 3,200 patients followed prospectively) in patients treated at doses in a range of 300-450 mg/day. This seizure incidence (0.4%) may exceed that of some other marketed antidepressants.
Additional data accumulated for the immediate-release formulation of bupropion suggested that the estimated seizure incidence increases almost 10-fold between 450 and 600 mg/day. The 600 mg dose is twice the usual adult dose and 1⅓ the maximum recommended daily dose (450 mg) of Wellbutrin XL. This disproportionate increase in seizure incidence with dose incrementation calls for caution in dosing.
Patient Factors: Predisposing factors that may increase the risk of seizure with bupropion use include history of head trauma or prior seizure, central nervous system tumor, the presence of severe hepatic cirrhosis and concomitant medications that lower seizure threshold.
Clinical Situations: Circumstances associated with an increased seizure risk include, among others, excessive use of alcohol or sedatives (including benzodiazepines); addiction to opiates, cocaine or stimulants; use of over-the-counter stimulants and anorectics; and diabetes treated with oral hypoglycemics or insulin.
Concomitant Medications: Many medications (eg, antipsychotics, antidepressants, theophylline, systemic steroids) are known to lower seizure threshold.
Recommendations for Reducing the Risk of Seizure: Retrospective analysis of clinical experience gained during the development of bupropion suggests that the risk of seizure may be minimized if the total daily dose of Wellbutrin XL does not exceed 450 mg; and if the rate of incrementation of dose is gradual.
Wellbutrin XL should be administered with extreme caution to patients with a history of seizure, cranial trauma or other predisposition(s) toward seizure or patients treated with other agents (eg, antipsychotics, other antidepressants, theophylline, systemic steroids, etc) that lower seizure threshold.
Hepatic Impairment: Wellbutrin XL should be used with extreme caution in patients with severe hepatic cirrhosis. In these patients, a reduced frequency and/or dose is required as peak bupropion as well as AUC levels are substantially increased and accumulation is likely to occur in such patients to a greater extent than usual. The dose should not exceed 150 mg every other day in these patients (see Dosage & Administration, Precautions, and Pharmacology: Pharmacokinetics under Actions).
Angle-Closure Glaucoma: The pupillary dilation that occurs following use of many antidepressant drugs, including Wellbutrin XL, may trigger an angle closure attack in a patient with anatomically narrow angles who does not have a patent iridectomy.
Potential for Hepatotoxicity: In rats receiving large doses of bupropion chronically, there was an increase in incidence of hepatic hyperplastic nodules and hepatocellular hypertrophy. In dogs receiving large doses of bupropion chronically, various histologic changes were seen in the liver and laboratory tests suggesting mild hepatocellular injury were noted.